EHR Terms Every Ambulatory Provider Should Know
If you work in an ambulatory practice, you already know that an EHR can feel a little like a second language. There are menus, acronyms, data fields, workflows, integrations, reports, and compliance terms flying around everywhere.
Some of them are obvious; some sound like they were invented in a meeting no one fully agrees happened; and some matter more than most providers realize. Research on
semantic-driven data quality improvements in EHRs highlights that standardized language and coding frameworks can enhance both clinical decision support and data integrity.
To help with this, we have curated an EHR glossary with important terms that form the foundation of modern medical practice. Whether you are considering a new system or looking to enhance your current workflows, this guide will provide clarity. We will explore the key concepts, why they matter to your practice, and how they connect to the comprehensive solutions Meditab offers.
Understanding Core EHR Terms
Mastering this electronic health record terminology is far from a minor administrative exercise. The software framework you deploy impacts your clinical documentation workflows, patient retention, compliance audits, and financial collections. When your clinical or billing teams do not fully comprehend these underlying EHR terms, your practice risks workflow friction, billing rejections, and misaligned patient engagement paths.
Whether you’re a solo practitioner, part of a multi-specialty group, or running a busy ambulatory clinic, understanding the EHR terminologies listed below will help you make the most of your technology, improve patient care, and run a smoother practice.
The Foundations of Ambulatory Health IT
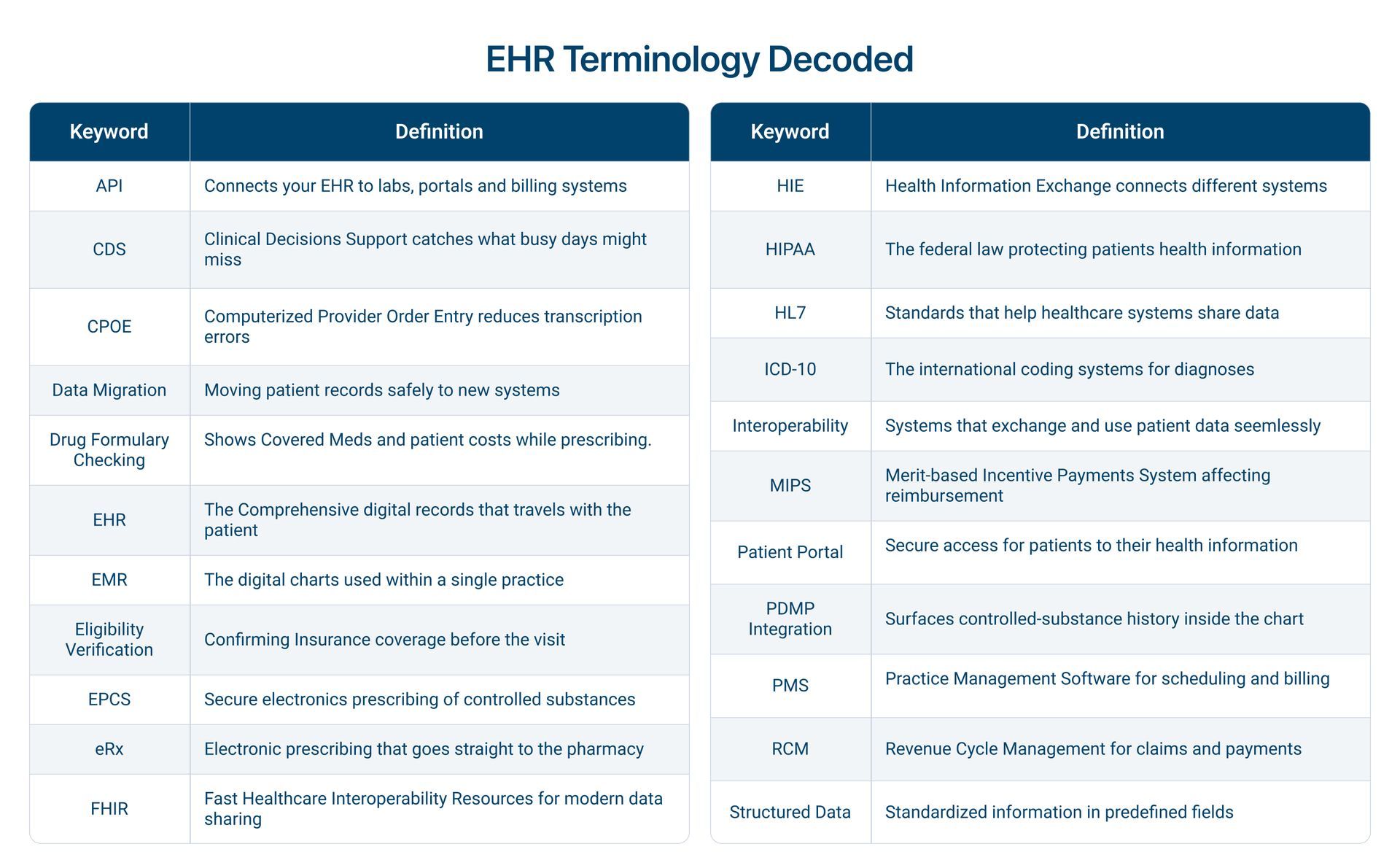
Below is a provider-friendly breakdown of common terms you are likely to see in your EHR, practice management, or connected health systems.
1. API (Application Programming Interface)
An API is a tool that allows two software systems to talk to each other. APIs help your EHR connect to labs, patient portals, billing systems, and other technologies without creating manual work for staff.
2. Clinical Decision Support (CDS)
Tools built into the EHR that surface relevant knowledge at the point of care. These are alerts for drug interactions, reminders for overdue screenings, and condition-specific guidance. No provider can hold every guideline and interaction in their head. CDS acts as a quiet second set of eyes, catching the things a busy day might otherwise let slip. Used well, it improves safety; the art is in tuning it so it helps without causing alert fatigue.
3. Clinical Documentation
The process of recording a patient’s medical history, symptoms, examination findings, diagnosis, and treatment plan within the EHR. Accurate clinical documentation supports better coding, billing, compliance, and continuity of care. Poor documentation is one of the leading causes of claim denials. Learn more in our article on clinical documentation and its importance.
4. Computerized Provider Order Entry (CPOE)
The electronic entry of orders, including medications, labs, imaging, and referrals, directly into the system, replacing handwritten or verbal orders. CPOE removes the ambiguity of handwriting and the gaps of verbal relay, and it lets the system check each order against the patient's record in real time. Fewer transcription errors mean safer care.
5. Data Migration
The meticulous process of transferring digital health records, patient demographics, clinical documentation histories, and patient insurance information from an outdated, legacy software database into a new, modern software platform. Switching to a superior software system shouldn't mean losing decades of hard-earned patient histories.
Executing a clean transition requires a deep technical understanding of data mapping and validation. A complete guide to
data migration in healthcare helps practices minimize clinic downtime, prevent data loss, and maintain strict record compliance during a software upgrade.
6. Electronic Health Record (EHR)
An Electronic Health Record is a digital version of a patient’s medical history, including diagnoses, medications, treatment plans, and test results. EHRs are the backbone of modern ambulatory care. A well-designed system improves care coordination, reduces errors, and enhances productivity. If you're exploring options, this complete guide on EHR software is a great starting point.
7. Electronic Medical Record (EMR)
An EMR is the digital chart created within a single practice for that practice's own use. The distinction is subtle but real: an EMR is essentially the record's "local" version, while an EHR is the shareable, interoperable version meant to move between organizations. The terms are constantly swapped in casual conversation, but the difference signals intent. If your software is truly an EHR, it's built to connect and exchange in a world that increasingly rewards data sharing.
8. Eligibility Verification
The process of confirming a patient's insurance coverage and benefits before the visit, ideally automatically through the Practice Management (PM) system. Verifying eligibility upfront prevents the nasty downstream surprise of a denied claim or a patient being billed for a service they thought was covered. It's a small step that protects both the patient relationship and the practice's cash flow.
9. EPCS (Electronic Prescribing of Controlled Substances)
A specialized, highly secure electronic prescription workflow that permits healthcare providers to electronically write, sign, and transmit prescriptions for controlled substances (Schedules II-V) directly to pharmacies. Managing controlled substance workflows mandates strict regulatory compliance to combat fraud and substance abuse. EPCS platforms require certified systems with robust two-factor authentication and identity verification. Using an electronic system for controlled substances eliminates traditional paper-based risks, ensures strict legal compliance with federal DEA mandates, and provides an unalterable digital audit trail for public health audits.
10. E-Prescribing (eRx)
Electronic Prescribing, or eRx, is a feature that enables secure, bidirectional electronic communication of information between practitioners and pharmacies. This allows providers to send prescriptions directly to a patient's pharmacy of choice from within their EHR.
Modern eRx platforms like Meditab’s IMS also include features for checking drug interactions, allergies, and formulary information in real time. E-prescribing is a standard of care. It significantly reduces medication errors associated with illegible handwriting, eliminates the need for paper prescriptions that can be lost or forged, and speeds up the process for patients. This is a direct application of the EHR’s capabilities to improve patient safety.
11. Drug Formulary Checking
An automated software capability that queries an insurance payer’s official list of covered medications and tier parameters in real time during the clinical prescribing window. Prescribing a medication that is non-formulary or sits on an expensive tier leads to immediate pharmacy rejections and treatment non-adherence. Real-time drug formulary checking allows providers to view patient-specific out-of-pocket costs and tier requirements directly on their screens. This transparency allows clinicians to immediately select covered therapeutic alternatives, preventing unexpected post-visit phone tag and pharmacy delays.
12. FHIR
FHIR stands for Fast Healthcare Interoperability Resources, a modern standard for sharing healthcare information. FHIR is built for faster, more flexible communication between systems. Meditab’s article on HL7 FHIR API and how it improves interoperability explains why this matters so much for connected care.
13. Health Information Exchange (HIE)
Health Information Exchange is the process of electronically mobilizing healthcare information across organizations within a region, community, or hospital system. It is the infrastructure that allows different EHR systems to communicate with one another.
An HIE enables the electronic transfer of clinical information between disparate systems while preserving the meaning of the information exchanged. HIE is the practical application of interoperability. For an ambulatory practice, an HIE eliminates the frustration of faxing records or waiting for CDs to arrive in the mail.
It enables the secure, electronic transfer of patient information directly into your system. This is crucial for a seamless patient experience, as you can receive admission and discharge notes, as well as consultations, electronically.
Meditab's health information exchange product is designed to simplify this process, ensuring your practice stays connected to the broader healthcare ecosystem.
14. HIPAA (Health Insurance Portability and Accountability Act)
A landmark US federal law enacted in 1996 that established strict national standards to protect sensitive patient health information from being disclosed without a patient's consent or knowledge, enforced through the HIPAA Privacy and Security Rules.
Data breaches and privacy violations can lead to massive federal fines, devastating legal liabilities, and the complete loss of community trust. Every component of your digital architecture, from internal text chat modules and telehealth portals to your billing database, must utilize enterprise-grade encryption and secure access logs to protect patient privacy at all times.
15. HL7
HL7 is a set of standards that helps healthcare systems share and interpret data. It is one of the foundations of smooth data exchange between systems. Providers benefit when labs, referrals, and patient records move cleanly across platforms.
16. ICD-10
The international coding system is used to classify diagnoses. Every condition the provider treats is assigned a standardized ICD-10 code. These codes are used to communicate the reason for care to payers and to track it across the health system. Accurate diagnosis coding is the difference between a clean claim and a denied one, and it feeds the data used for population health and quality reporting.
17. Interoperability
The ability of different EHR systems and health IT tools to swiftly exchange and use patient data. True interoperability in healthcare reduces friction when referring patients or receiving records from hospitals and labs. Meditab’s support for standards like HL7 FHIR makes sharing information faster and more reliable. Read more in our guide on HL7 FHIR API and how it improves interoperability.
18. MIPS (Merit-based Incentive Payment System)
Programs that incentivize providers to use EHRs effectively to improve patient outcomes. MIPS matters a lot because compliance affects reimbursement and performance scores. Read more about
understanding MIPS and Medicare's Quality Payment Program.
19. Patient Engagement Software
Tools that help patients actively participate in their care through portals, appointment reminders, educational materials, and secure messaging. Strong patient engagement leads to better adherence, higher satisfaction, and improved outcomes.
Meditab’s patient engagement software makes it easy to keep patients connected.
20. Patient Engagement Tools
Digital tools that enable patients to interact with their healthcare providers (e.g., portals, reminders, messaging). Better engagement leads to improved adherence and satisfaction.
21. Patient Portal
A
patient portal is a secure website or app where patients can view their health information, request appointments, see results, and message the practice. This is crucial because the portal turns patients from passive recipients into active participants. It cuts down on phone tag, speeds up routine communication, and patients increasingly expect it as a baseline convenience.
22. PDMP (Prescription Drug Monitoring Program) Integration
A native software connection that links an EHR directly to a state's electronic database, tracking real-time controlled substance prescriptions written and dispensed within that specific state. Logging out of an EHR to check a separate state database drastically slows down clinical workflows and contributes heavily to provider software fatigue. Seamless PDMP integration instantly surfaces a patient's comprehensive controlled-substance history within their active medical chart. This functionality ensures that providers can screen for drug-seeking behaviors and make safe, informed prescribing choices in seconds without disrupting the patient encounter.
23. Practice Management System (PMS)
A comprehensive administrative software solution that handles the non-clinical, operational side of a medical practice, including patient scheduling, demographic data collection, insurance eligibility verification, and financial billing workflows. Clinical excellence requires a stable operational foundation.
When your clinical records are disconnected from your scheduling system, double data entry and human billing errors multiply. Deploying an all-in-one system that unifies clinical charting with intelligent
practice management software ensures that when a receptionist checks a patient in, their demographic records, active insurance copays, and clinical charts are instantly aligned for the provider.
24. Revenue Cycle Management (RCM)
The financial process for managing claims, payments, and revenue. Efficient RCM ensures timely reimbursements and reduces claim denials. Learn more about our Revenue Cycle Management.
25. Structured vs. Unstructured Data
Structured data refers to standardized information entered into predefined fields within a database, such as selecting a diagnostic ICD-10 code from a dropdown menu, checking specific symptom boxes, or logging numeric vitals.
Unstructured data refers to free-form information that does not conform to a strict database model, such as dictated narrative notes, typed clinical descriptions, or scanned external PDF consult letters. While narrative typing provides rich context, structured data is what drives modern practice automation.
When data is structured, your system can run population health metrics, trigger automated medication interaction alerts, and auto-populate billing templates. Balancing these elements is essential for maximizing the value of your clinical documentation and its importance to the long-term continuity of care.
In A Nutshell
Navigating the terminology of electronic health records can be a challenge, but it is a critical step toward unlocking the full potential of your practice’s technology. Understanding these terms is not just about speaking the language; it's about making better business decisions. By becoming fluent in this electronic health record terminology, you empower your practice to select an intelligent, integrated system, one that supports clinical excellence, operational efficiency, and a healthy bottom line.
This EHR glossary contains essential terms, providing a solid foundation while the complexity of healthcare technology continues to grow. Understanding distinctions, such as the fact that EMRs are for internal use while EHRs are meant for sharing across the entire care continuum, is key to making the right choice for your practice. It is crucial to see how each term fits into your practice's ecosystem. A modern EHR is more than just a digital filing cabinet; it is a comprehensive suite of tools that includes practice management, revenue cycle management, and patient engagement.
By investing time in understanding these concepts, you are not just preparing for the future; you are optimizing your practice for today. Meditab’s robust IMS is an EHR that serves as a central hub, connecting various facets of your business, from clinical workflows to financial management. It allows fast health information exchange and proactive care management, ensuring your practice remains at the forefront of the healthcare industry.
Schedule a Consultation for me.
FAQs
What is an EHR glossary?
An EHR glossary is a collection of commonly used EHR terms and definitions that help providers understand EHR terminology and use their systems effectively.
What is the difference between a standalone ambulatory EHR and a modular system?
A standalone or all-in-one ambulatory EHR integrates clinical charting, scheduling, practice management, and billing into a single, cohesive database engine from day one. A modular approach combines disparate software systems from multiple independent vendors, requiring custom API connections or HL7 bridges to communicate across platforms.
What is the difference between an EMR and an EHR?
An EMR is the digital chart a single practice creates and uses internally, while an EHR is the broader, shareable record designed to move between different providers and settings. In everyday conversation, the terms are used interchangeably. Still, the distinction matters because it signals whether the system is built to connect and exchange data, a capability that matters more every year.
What does interoperability mean in healthcare?
Interoperability is vital because it enables different healthcare systems to communicate with one another. For an ambulatory practice, this means you can receive lab results, consult notes, and other patient data electronically and directly into your EHR. This improves care coordination, reduces duplicate testing, minimizes manual data entry errors, and saves time.
Why should providers learn EHR terms?
Understanding EHR terms helps improve documentation accuracy, enhance workflows, and ensure compliance with healthcare regulations.
Share this post: